Mental Health is a Spectrum
Mental Health Belongs to All of Us
If someone asked you about your physical health today, you wouldn't pause to consider whether the question applied to you. Of course it does. You have a body, and that body has a state of health right now — perhaps you slept well, perhaps your back aches, perhaps you're recovering from a cold, perhaps you feel strong. Your physical health is not a fixed label. It is a living, moving condition that changes day by day, hour by hour, across your lifetime.
Mental health is no different. And yet, for reasons we will unpick throughout this course, many of us have grown up treating mental health as something other people have — something you only think about when something has gone wrong. We talk about mental illness as if it were a discrete category of people, separate from the rest of us going about our ordinary lives. This framing is not only inaccurate; it is one of the single greatest barriers to early help-seeking, recovery and a humane workplace culture.
So let's begin this course by retiring that framing entirely. The foundational idea we want you to carry into every conversation, every policy decision, every cup of tea with a colleague, is this: everyone has mental health, all of the time, and it sits somewhere on a continuum that shifts throughout life.
The continuum: a more accurate map
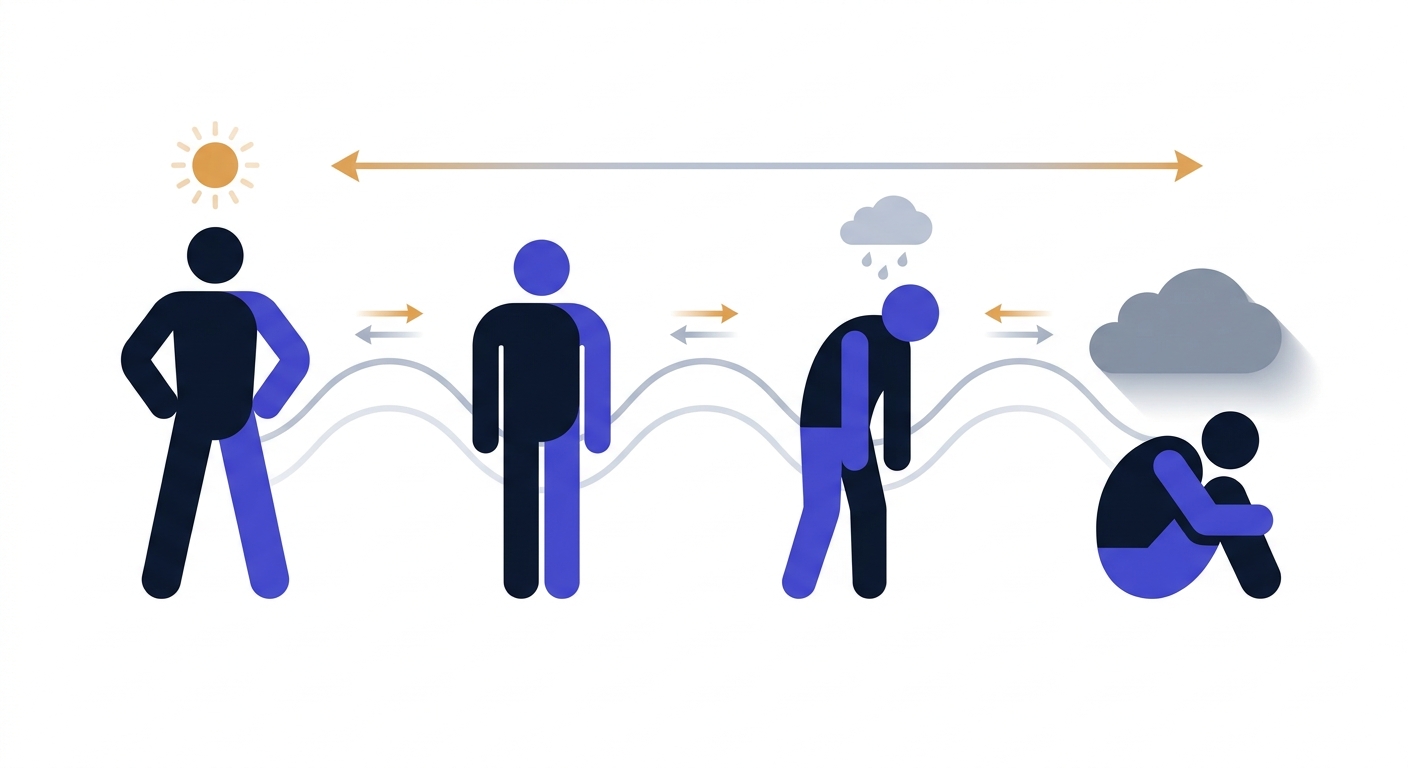
Picture a horizontal line. On the far left, imagine someone thriving — energised, sleeping well, engaged in their work and relationships, able to weather setbacks. Moving rightward, we pass through coping (steady, getting on with life, occasional dips), then struggling (visibly stretched, sleep disrupted, mood lower, productivity dropping), and finally unwell (significantly impaired, perhaps with a diagnosed condition, possibly unable to function in usual roles).
Crucially, the arrows on this continuum point both ways. People do not start at the left and travel inexorably to the right. We oscillate. A person who has been clinically depressed can return to thriving. A person currently thriving can find themselves struggling within weeks after a bereavement, a relationship ending, a difficult restructure at work, or for reasons that aren't immediately clear at all. This is not failure. This is being human.
Everyone has mental health — it moves along a continuum from thriving to struggling to unwell, and back. It is not us and them.
What Each Zone Looks Like at Work
Abstract models are useful, but they only become powerful when you can recognise them in the texture of an ordinary working week. Let's walk through each zone with the kind of detail that makes it usable on a Monday morning.
Thriving
A colleague in the thriving zone isn't necessarily euphoric or untroubled. Thriving is not the absence of difficulty — it is the presence of capacity. The person sleeps reasonably well most nights. They feel connected to people who matter to them. They can concentrate on work that requires effort, take pleasure in small things, recover from a hard meeting by lunchtime, and absorb a piece of critical feedback without it derailing their week.
At work, you might notice: they contribute ideas in meetings, they accept stretch assignments with curiosity, they laugh easily with colleagues, they take their annual leave and return refreshed, and they tend to support others who are struggling. Importantly, thriving people still have bad days. The difference is that a bad day stays a bad day rather than becoming a bad fortnight.
Coping
This is where most of us spend a great deal of our working lives, and it is not a problem in itself. Coping looks like ordinary competence under ordinary pressure. The deadline is tight but achievable. The commute is tiring but manageable. There is a niggling worry about a parent's health, or a tax return, or a difficult conversation pending with a teenager, but it does not consume the day.
People in the coping zone get the job done. They may be a little less playful than usual, a little quicker to decline a social invitation, a little more reliant on caffeine or a glass of wine in the evening. They are running close to the edge of their reserves but they are still inside them. The risk in this zone is that it can be invisible — both to others and to the person themselves. We tend to think "I'm fine" when what we really mean is "I am managing." The two are not the same.
Struggling
This is where the early signs of a mental health problem become observable, often first to others before the person themselves can name what is happening. Sleep becomes unreliable — either too little or too much. Concentration frays; the person rereads the same paragraph three times. Small irritations become large ones. Joy dims. Tasks that were once routine begin to feel like climbing a hill in heavy boots.
At work, you might see: missed deadlines from someone who normally hits them, withdrawal from team chat, a usually punctual person arriving late, declining the team lunch they would have enjoyed, more sick days clustered together, errors in familiar tasks, or a flatness in tone where there used to be warmth. The person may say they are tired, or stressed, or run-down. They may not yet have the language — or the safety — to say more.
This is the zone where workplace awareness matters most. The struggling zone is not a crisis, but it is the point at which timely, compassionate attention can prevent the slide into the unwell zone. We will spend a great deal of this course building your confidence to notice and to act here.
Unwell
At the far end of the continuum, a person is significantly impaired by their mental health. They may have a diagnosed condition — depression, an anxiety disorder, PTSD, bipolar disorder, an eating disorder. They may be receiving treatment, or they may not yet have sought help. Daily functioning is difficult: getting out of bed, eating, washing, leaving the house, holding a conversation. Work, if it is happening at all, requires enormous effort and may be impossible to sustain.
It is critical to understand that being in the unwell zone is not a moral failing, a weakness of character, or an inability to "think positive." It is a health condition, as real and as treatable as a broken leg or asthma. And — this is the bit the continuum model insists on — people return from this zone. With the right support, treatment, time and conditions, people move back through struggling, into coping, and into thriving. Recovery is the rule, not the exception.
Movement is the point
Notice that we have described zones, not types of people. Nobody is a struggling person. Somebody is struggling, right now, in this season of their life, for reasons that may or may not be visible to you. Six months from now they may be thriving. Six months ago they may have been thriving. The continuum is a map of states, not a taxonomy of people. This distinction matters enormously, because the moment we start to categorise colleagues as "the anxious one" or "the depressed one," we have stopped seeing them and started filing them.
Reflection exercise: map your own year
Take five minutes — genuinely, set a timer — and sketch your own continuum on a piece of paper. Mark, honestly, where you have been at three or four points over the past twelve months. Perhaps you were thriving in the spring, slid into struggling during an autumn restructure, and are coping now. Perhaps the pattern is different.
Then ask yourself two questions:
- What moved me along the line? Was it work pressure, a relationship, sleep, a health issue, a loss, a change of circumstance, something I cannot quite name?
- What helped me move back toward thriving? A conversation with a specific person? Time outdoors? Reducing alcohol? Asking for help? A holiday? Therapy? Changing something at work?
This is not idle reflection. The patterns you notice in yourself are the same patterns you will learn to recognise — with appropriate humility — in others. And the things that help you move back are part of the toolkit you can quietly model and offer to colleagues.
Why the Spectrum Model Changes Everything
It would be easy to treat the continuum as a neat diagram and move on. But the implications of taking it seriously are profound, and they reshape how we behave at work.
It dissolves "us and them"
If everyone has mental health, then there is no separate population of "people with mental health issues" to be supported by the rest of us who are, by implication, fine. There is just us — a workforce of human beings, each somewhere on the line, each moving, each occasionally needing more support and occasionally able to offer it. The Mental Health First Aider, the manager, the CEO and the new starter are all on the same continuum. This levelling is the foundation of any culture in which people feel safe to speak up.
It legitimises early help-seeking
The traditional model — you are either ill or you are not — encourages people to wait until they are visibly unwell before they ask for help. By then, recovery is harder and longer. The spectrum model says: the moment you notice you are sliding from coping into struggling is exactly the moment to do something. That "something" might be small — a conversation, a walk, a GP appointment, a quiet word with your manager about workload. Early action is high-leverage action.
It reframes recovery as normal
Because the continuum has arrows pointing both ways, returning from unwell to thriving is not a miracle — it is the expected trajectory with the right conditions. This matters for the person recovering, who needs to believe it is possible. It matters for colleagues, who need to expect and welcome that return rather than treating the person as permanently fragile. And it matters for organisations, which need to design return-to-work processes that assume recovery, not chronicity.
It connects mental and physical health
The same model applies to physical health, and the two are deeply intertwined. Poor sleep affects mood. Chronic pain depletes resilience. Depression suppresses the immune system. Exercise improves mental health. The person who has been signed off with back pain may also be sliding into the struggling zone mentally — and vice versa. Treating mental health as a separate domain, walled off from physical health, misses how human beings actually work.
It makes compassion practical
Perhaps most importantly, the spectrum model turns compassion from a vague virtue into a concrete practice. If you accept that the colleague who snapped at you in a meeting may be struggling, that the team member missing deadlines may be unwell, that the high performer who has gone quiet may be sliding from coping into something harder — then your default response shifts. You ask before you assume. You check in before you escalate. You offer presence before you offer advice. None of this requires you to be a clinician. It requires you to remember that the person in front of you is on the same continuum as you, just at a different point today.
A note on language
You will hear many phrases used in this space — mental health, mental illness, mental ill-health, mental wellbeing, mental health problem, mental health condition. We will use these carefully throughout the course, but for now hold this distinction: mental health is the universal property everyone has; mental ill-health, a mental health problem or a diagnosed mental health condition describe specific points further along the continuum. Using "mental health" as a synonym for "mental illness" is one of the small linguistic habits that keeps the us-and-them framing alive. Once you start to notice it — in headlines, in policies, in your own speech — you will not be able to unnotice it.
Key takeaway
The spectrum in one paragraph: Mental health is universal. It moves along a continuum from thriving, through coping and struggling, to unwell — and back again. People are not their position on the line; they are travellers along it. Recognising this dissolves the false divide between "healthy" colleagues and "unwell" ones, legitimises early conversations, normalises recovery, and turns compassion into something we practise every day rather than something we reserve for emergencies.
What this means for you at work: notice movement, not labels. Ask how someone is, and ask twice. Treat your own position on the continuum with the same honesty you would treat a colleague's. And remember that the most useful thing you can offer is rarely expertise — it is your willingness to see another human being clearly, exactly where they are today.
Carrying This Forward
In the next lesson, we will sharpen our vocabulary further by distinguishing between everyday stress, a mental health problem, and a diagnosed condition. Each of these sits at different points on the spectrum we have just mapped, and being able to tell them apart — without slipping into amateur diagnosis — is one of the most useful skills you will develop in this course.
Before you move on, sit for a moment with the central reframe of this lesson. Mental health is not something a minority of people have. It is something all of us have, all of the time. The colleague you find difficult, the senior leader who seems unflappable, the new joiner who hasn't said much, you, your line manager, your CEO — every one of us is on the line. The line moves. That is the whole picture. Everything else in this course builds on it.
Enjoyed this preview? Enrol to unlock all 44 lessons + your certificate.
Training a team? Buy seats for your team →